Male pattern baldness affects millions of men worldwide, and understanding where you stand on the progression scale is crucial for choosing the right treatment. Norwood 2 hair loss represents one of the earliest visible stages of male pattern hair loss, characterized by a receding hairline at the temples. This stage offers the best opportunity for intervention, whether through medical therapies or surgical procedures.
The Norwood scale serves as the gold standard for classifying male pattern baldness, helping both patients and medical professionals determine the severity of hair loss and plan appropriate treatment strategies. At this early stage, men have multiple options ranging from non-invasive medications to advanced hair transplant techniques.

Understanding Norwood 2 Hair Loss
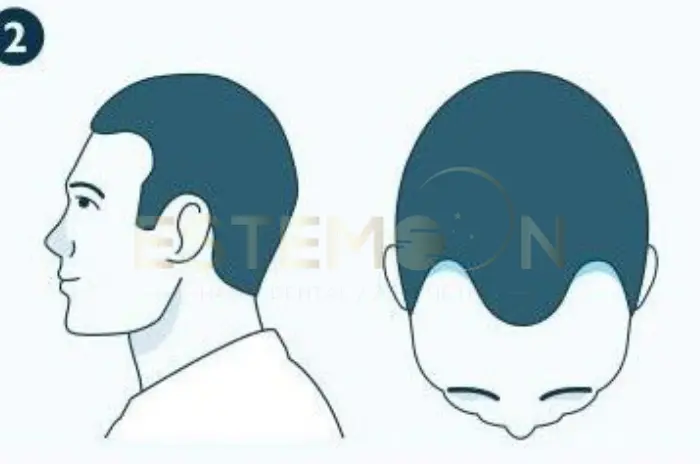
Norwood 2 hair loss marks the beginning of noticeable male pattern baldness, though many men may not recognize it as such. At this stage, the hairline begins to recede slightly at the temples, creating a triangular recession that typically extends no more than 2 centimeters above the natural crease of the upper brow. This creates what’s often called a mature hairline rather than full baldness.
The condition results from androgenetic alopecia, a genetic sensitivity to dihydrotestosterone (DHT), a hormone derived from testosterone. Hair follicles in the temple regions contain more androgen receptors, making them particularly vulnerable to DHT’s miniaturizing effects. Over time, these follicles produce progressively thinner and shorter hairs until they eventually stop producing visible hair altogether.
Many men wonder is Norwood 2 balding or simply a natural progression of aging. The answer depends on several factors including age, family history, and the rate of progression. Men in their late teens or early twenties showing Norwood 2 characteristics are more likely experiencing the onset of pattern baldness. However, men developing this hairline pattern in their thirties or later may simply be experiencing a normal mature hairline that won’t progress further.
The receding hairline at Norwood 2 typically maintains symmetry, with both temples receding at similar rates. The frontal hairline may remain relatively intact, though it often sits higher than in adolescence. Early detection at the Norwood stage 2 provides significant advantages, as hair follicles haven’t completely miniaturized and can still respond to medical treatments.
Hair Growth Therapies for Norwood 2
Medical treatments offer the first line of defense against Norwood 2 hair loss progression, and early intervention significantly improves long-term outcomes. Medications for Norwood 2 work by targeting the underlying hormonal mechanisms that cause follicle miniaturization.
Finasteride treatment remains the most effective FDA-approved oral medication for male pattern baldness. This prescription drug inhibits the 5-alpha-reductase enzyme that converts testosterone into DHT, reducing scalp DHT levels by up to 70%. Studies show that approximately 90% of men who take finasteride daily experience either hair loss stabilization or regrowth. The standard dosage is 1mg per day.
Minoxidil for hair loss provides a complementary topical treatment available over-the-counter in 2% and 5% concentrations. This vasodilator increases blood flow to hair follicles and extends the anagen (growth) phase of the hair cycle. Applied twice daily to the affected areas, minoxidil can stimulate regrowth in miniaturized follicles and prevent further recession. The 5% foam formulation tends to be most effective for men with Norwood 2 receding hairline.
Low-level laser therapy (LLLT) offers a non-pharmaceutical option that uses red light wavelengths to stimulate cellular activity in hair follicles. FDA-cleared devices like laser caps can be used at home several times per week. While effects are generally modest compared to finasteride or minoxidil, LLLT has no systemic side effects.
Platelet-rich plasma (PRP) therapy involves drawing the patient’s blood, concentrating the growth factors, and injecting them into the scalp. This regenerative treatment stimulates dormant follicles and improves hair density. Multiple sessions spaced 4-6 weeks apart are typically required.
Combination therapy often yields superior results. The most common protocol pairs oral finasteride with topical minoxidil, addressing hair loss through both hormonal regulation and direct follicular stimulation.
The Norwood Hamilton Scale for Male Pattern Baldness
The Norwood scale, also known as the Norwood-Hamilton scale, provides a standardized classification system for male pattern baldness developed by Dr. James Hamilton in the 1950s and later refined by Dr. O’Tar Norwood in the 1970s. This system divides male pattern hair loss into seven primary stages.
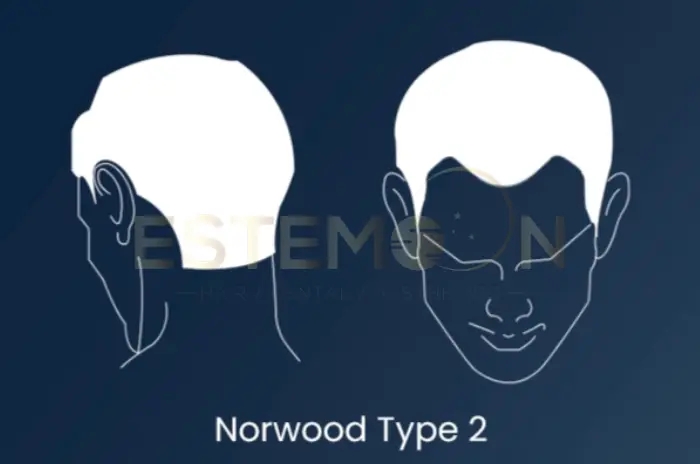
Norwood stage 2 specifically describes minimal recession at the temporal areas, forming a symmetrical M-shape when viewed from above. The hairline remains relatively frontal, and the vertex (crown) shows no thinning. This stage distinguishes itself from Norwood 1, where the hairline remains essentially juvenile, and Norwood 3, where temporal recession becomes more pronounced.
The scale recognizes two main progression patterns: the classic pattern and the Type A variant. In the classic Norwood 2 hair loss pattern, the temples recede while the frontal hairline remains relatively preserved. The Type A variant shows recession across the entire frontal hairline without deep temporal triangular recession.
Understanding your position on the Norwood scale helps predict future progression and treatment needs. Research indicates that men who reach Norwood 2 by their early twenties have a higher likelihood of progressing to advanced stages without intervention. Conversely, men who don’t develop Norwood 2 characteristics until their thirties often experience slower progression.
Medical professionals use standardized photographs and measurements to accurately classify patients. At Norwood stage 2, the measurement from the glabella to the hairline typically shows 1-2 centimeters of additional distance compared to a juvenile hairline.
Advanced Techniques in Norwood 2 Hair Transplants
Hair transplant Norwood 2 procedures offer permanent restoration for men who want to reverse their receding temples. Modern techniques provide natural-looking results with minimal scarring and downtime.
FUE hair transplant (Follicular Unit Extraction) represents the most popular method for addressing early-stage hair loss. This technique involves extracting individual follicular units from the donor area using micro-punches of 0.7-1.0mm diameter. These grafts are then transplanted into the receding temple areas. FUE leaves tiny dot scars that are virtually undetectable.
Direct Hair Implantation (DHI) refines the FUE process by using a specialized Choi implanter pen that combines graft placement and channel creation in one step. This technique allows surgeons to control the angle, direction, and depth of each transplanted hair with precision. The question of are FUE or DHI best for Norwood 2 transplants depends on individual factors including hair characteristics and surgeon expertise.
How many grafts for Norwood 2 varies based on the extent of temple recession and desired density. Most cases require 800-1,500 grafts to restore a natural-looking hairline and fill in the temple triangles. Conservative estimates suggest approximately 400-750 grafts per temple.
The hairline design process is crucial for natural hair transplant results. Skilled surgeons create irregular, asymmetric hairlines that mimic nature. Single-hair follicular units are placed at the very front, with two and three-hair units positioned behind to create density.
Sapphire FUE uses sapphire crystal blades instead of steel for creating recipient channels. These ultra-sharp blades create cleaner incisions with less tissue trauma, potentially improving healing times and graft survival rates.
Norwood 2 photos taken throughout the transplant process help patients understand expected timelines. The transplanted hairs shed within 2-4 weeks, then begin regrowing around month 3. Full results become apparent at 12-18 months.
Norwood 2 vs Norwood 3 Differences
Understanding the distinction between Norwood 2 vs Norwood 3 differences helps patients recognize when their hair loss has progressed. While both stages involve temple hair loss, the extent and impact differ significantly.
At Norwood stage 2, the temporal recession remains relatively shallow, typically 1-2 centimeters beyond what would be considered a mature hairline. Most men can still style their hair to completely conceal the minimal recession.
Norwood 3 shows deeper temporal recession extending 2-3 centimeters or more, creating more prominent M-shaped patterns. The temples become distinctly bare, making the recession visible even with styling efforts. Some men begin developing early crown thinning at this stage.
What is the main difference between Norwood 2 and 3 centers on both measurements and appearance. Norwood 3 represents the threshold where hair loss becomes cosmetically significant to most observers.
The progression timeline varies considerably. Some men remain at Norwood 2 indefinitely, while others progress to Norwood 3 within months. Questions like how long does Norwood 2 last don’t have universal answers, but most men without treatment see progression within 2-5 years.
Treatment strategies differ between these stages. Norwood 2 patients often achieve excellent results with medications alone. Norwood 3 patients more frequently require hair grafts Norwood 2 transplants to restore density.
Treatment Options for Norwood 2 Progression
Preventing Norwood 2 hair loss from advancing requires a strategic approach combining medical therapy and lifestyle modifications. The goal is maintaining the current hairline for decades.
Are medical treatments effective for Norwood 2 progression? The evidence strongly supports early intervention. Men who begin finasteride at Norwood 2 have approximately 85-90% success in preventing further recession over five years. Combining finasteride with minoxidil increases this success rate.
Lifestyle factors influence treatment success rates. Smoking constricts blood vessels in the scalp, reducing medication effectiveness. Managing stress through exercise and adequate sleep helps regulate hormones that may accelerate hair loss. Nutritional deficiencies in iron, vitamin D, or protein can compound genetic hair loss.
Monitoring progression allows timely treatment adjustments. Taking standardized photographs every 3-6 months under consistent lighting helps track subtle changes. Men who notice continued recession should consult their physician about adjustments.
Preventive transplants represent an emerging approach for young men with strong family histories. Rather than waiting for extensive loss, some patients undergo conservative hairline restoration at Norwood 2, then maintain results with medications.
Regular follow-up with dermatologists or hair restoration specialists ensures optimal treatment management. Annual check-ups allow assessment of medication side effects and evaluation of progression.
Norwood 2 Hair Loss Treatments Transplant Options Results – Frequently Asked Questions
What non-surgical growth therapies work for Norwood 2?
Finasteride and minoxidil are the most effective FDA-approved medical treatments, often combined with PRP therapy and low-level laser therapy for enhanced results.
Are FUE or DHI best for Norwood 2 transplants?
Both FUE and DHI provide excellent results for Norwood 2 receding hairline, with DHI offering slightly more precision in hairline design and FUE being more cost-effective.
What is the main difference between Norwood 2 and 3?
Norwood 2 shows minimal temple recession (1-2cm) that’s often concealable, while Norwood 3 displays deeper recession (2-3cm+) with clearly visible baldness.
Are medical treatments effective for Norwood 2 progression?
Yes, finasteride prevents further progression in 85-90% of men when started at Norwood stage 2, making early intervention highly effective for preservation.
Follow us on social media for updates, tips, and patient success stories:

